Dry AMD progression to GA is characterized by the development of new atrophic lesions, growth of individual areas, foveal encroachment, or coalescence of multiple lesions. GA can be detected using various imaging modalities, such as OCT and fundus autofluorescence (FAF), which are commonly available in most clinics.1-3,9
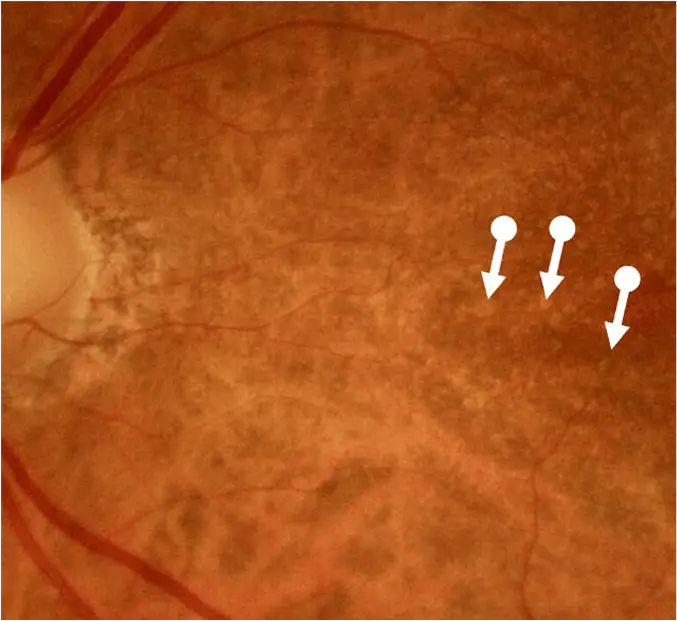
Although less sensitive for detecting early GA, color fundus photography can reveal GA lesions as hypopigmented areas with sharply demarcated borders. Fundus autofluorescence (FAF) is one of the primary modalities for detecting and monitoring GA. On FAF imaging, GA lesions appear as well-defined hypofluorescent (dark) areas due to loss of the retinal pigment epithelium (RPE). On OCT, characteristic features of GA include loss of the photoreceptors, loss of the RPE, and areas of choroidal hypertransmission, which appear as bright vertical columns with increased visualization of the underlying choroidal structures.1,3,4